V
O
K
A
Анатомия
Патологии
Статьи
Центр помощи
RU
Войти
Категории
Врожденные пороки сердца
Дефект межпредсердной перегородки, Тетрада Фалло, коарктация аорты
Стоматология
Кариес, патология пульпы, апикальный периодонтит, некариозные поражения
Приобретенные патологии сердца
Атеросклероз коронарных артерий, клапанные пороки сердца
Акушерство
Предлежание плода, предлежание плаценты, положение плода
Эмбриология
Бластоциста человека, эмбрион человека
Гинекология
Вагинит, эндометриоз, бартолинит, цервицит, лейомиома матки
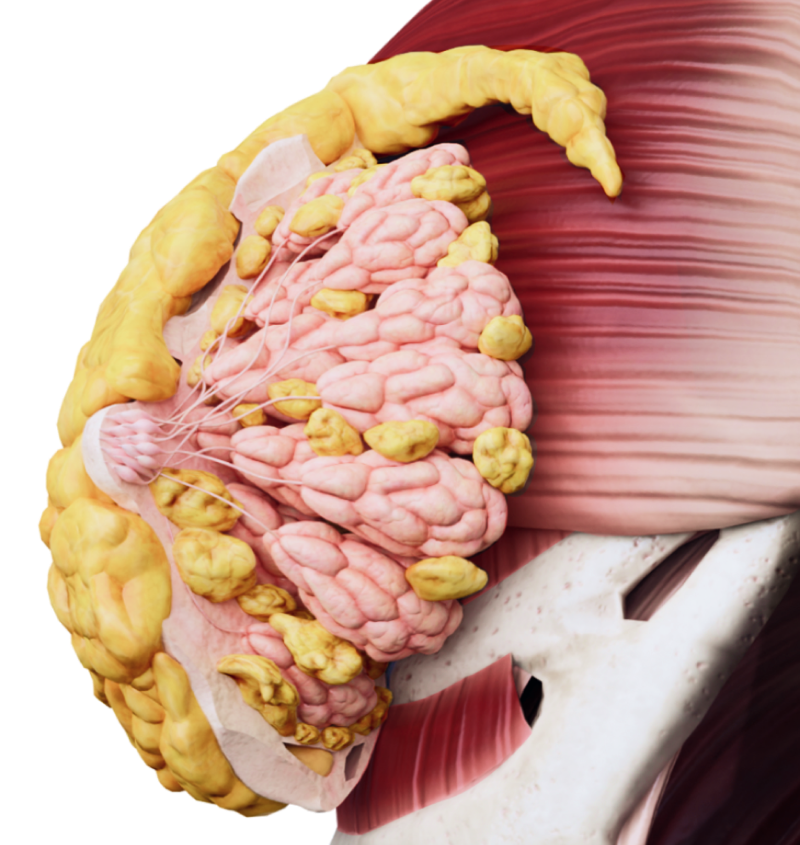
Образования молочных желез
Злокачественные образования молочной железы
Эндокринология
Аномалии развития щитовидной железы, зоб, гипертиреоз
Патологии ЦНС и ПНС
Субдуральные гематомы, эпидуральные гематомы, переломы костей черепа
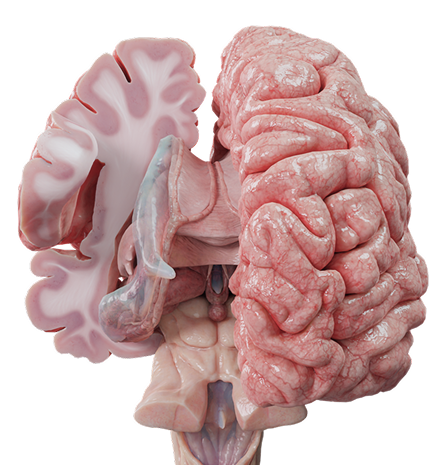
Онкология ЦНС и ПНС
Опухоли головного мозга и периферических нервов
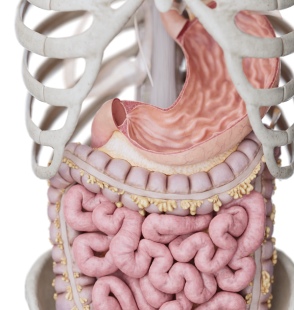
Болезни ЖКТ
Язва желудка, полипы желудка, язвенный колит
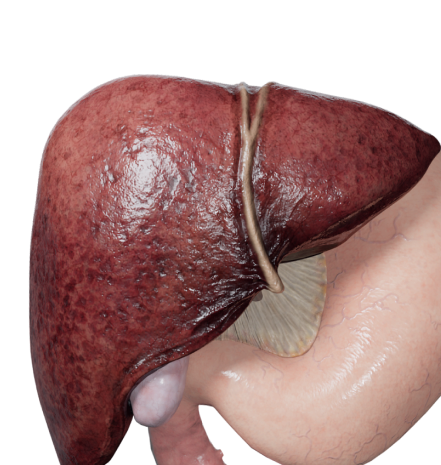
Болезни печени
Желчекаменная болезнь, цирроз печени, холециститы
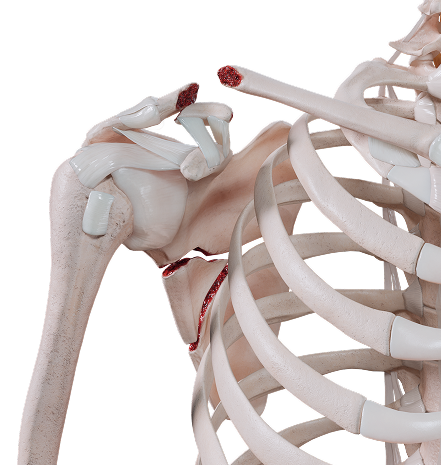
Травматология и ортопедия
Травмы позвоночника, травмы верхнего плечевого пояса
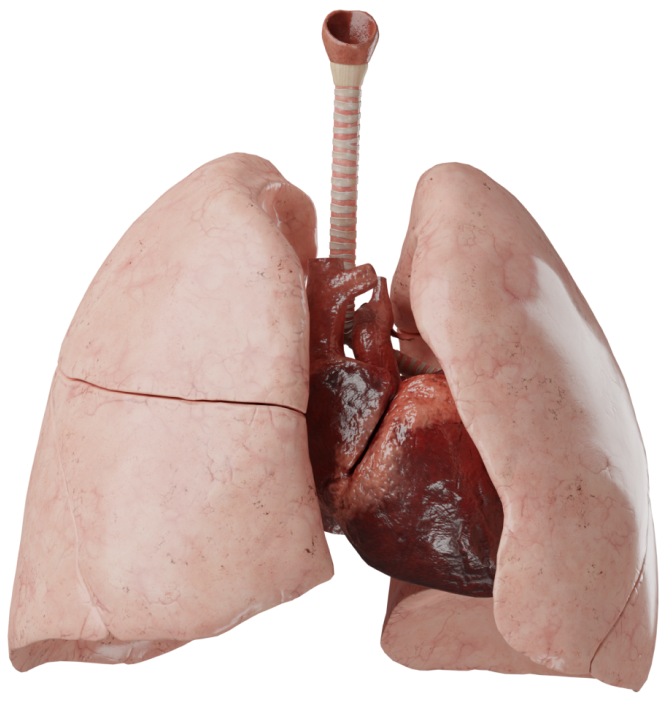
Болезни дыхательной системы
Гемоторакс, осложнения гемоторакса, пневмоторакс
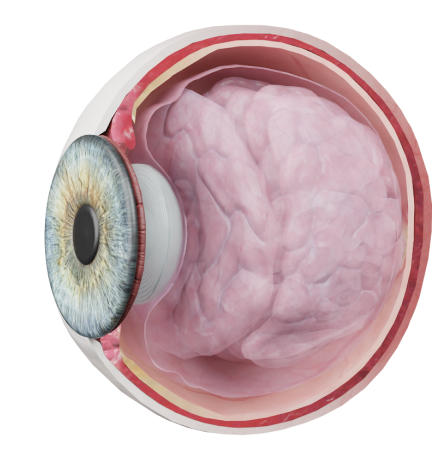
Патологии органов зрения
Конъюнктивит, дегенеративные заболевания конъюнктивы
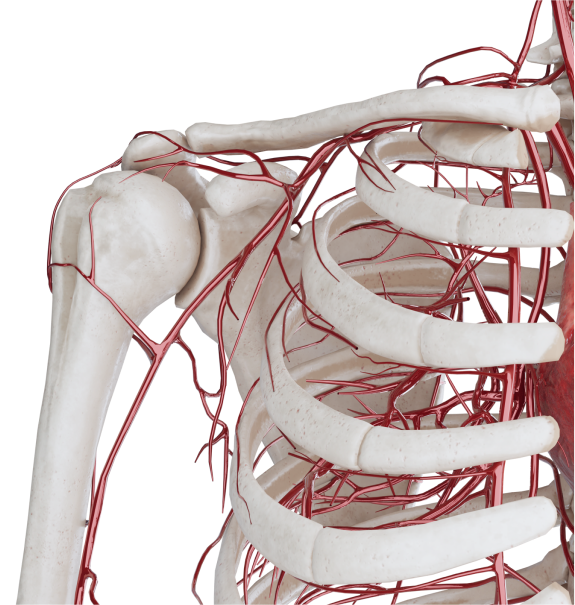
Патологии сосудистой системы
Аневризмы артерий, атеросклероз, болезни вен
Оториноларингология
Аномалии развития наружного уха, травмы наружного уха
Дерматология
Пятно, узелок, узел, пузырек
Назад
К патологии
Содержание
К патологии