V
O
K
A
Anatomy
Pathology
Articles
Help center
EN
Log In
Categories
Congenital Heart Defects
Atrial septal defect, Tetralogy of Fallot, Coarctation of the aorta
Dentistry
Caries, Pulp pathology, Apical periodontitis, Non-carious lesions
Acquired Heart Diseases
Coronary arteries atherosclerosis, Valvular heart disease, Cardiomyopathy
Obstetrics
Fetal presentation, Placenta previa, Fetal lie
Gynecology
Vaginitis, Bartholinitis, Cervicitis, Endometriosis, Leiomyoma of the uterus
CNS and PNS Disorders
Epidural hemorrhage, Subdural hemorrhage, Skull fractures
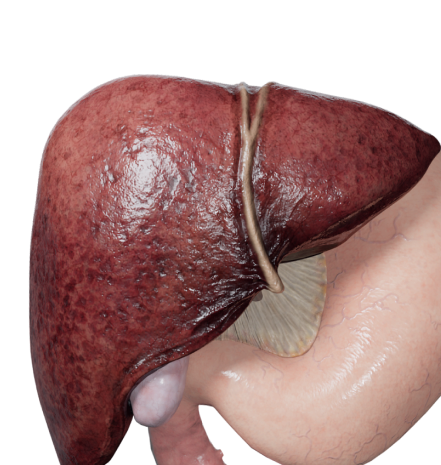
Liver Diseases
Cholelithiasis, Hepatic cirrhosis, Cholecystitis
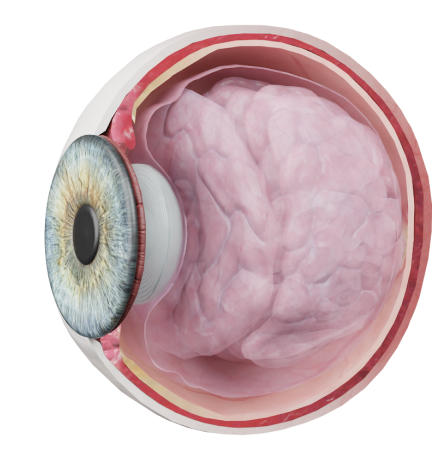
Eye Disorders
Conjunctivitis, Degenerative disorders of conjunctiva
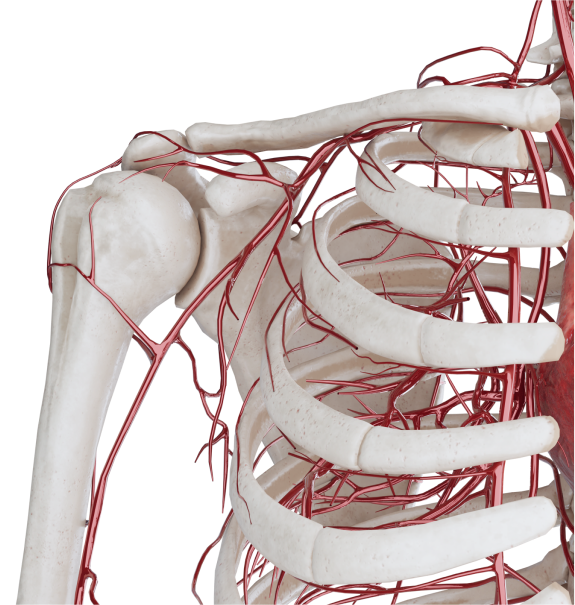
Vascular Diseases
Arterial aneurysms, Atherosclerosis, Venous diseases
Otorhinolaryngology
Developmental abnormalities of the external ear, External ear injuries
Back
Go to pathology
Table of contents
Go to pathology